Tumour Markers
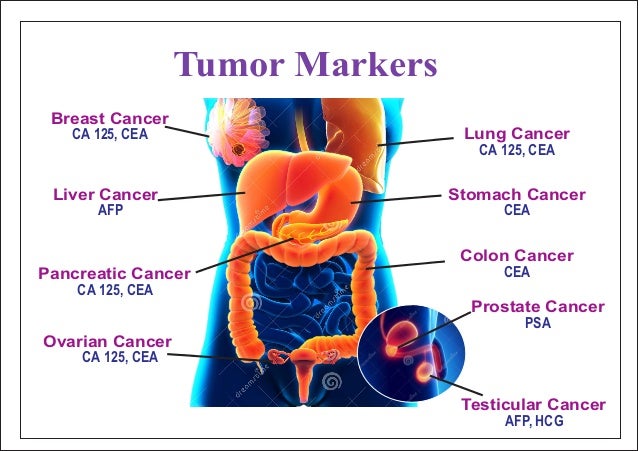
These are usually glycoproteins (soluble molecules) in the blood, which can be detected by monoclonal antibodies. Highly raised levels of a tumour marker can provide helpful information but inappropriate use can have economic implications and cause patients additional anxiety and distress. Additionally, unnecessary investigations may be associated with side-effects and may delay correct diagnosis and treatment.
Each tumour marker has a variable profile of uses:
Screening
Screening tests require high sensitivity to detect early-stage disease. No tumour marker has yet demonstrated a survival benefit in randomised controlled trials of screening in the general population.
Disease staging
For determining diagnosis and prognosis.
Assessing response to therapy
- Tumour marker values returning to normal may indicate cure despite radiographic evidence of persistent disease.
- In this circumstance, the residual tumour is often non-viable.
- Conversely, tumour marker levels may rise after effective treatment (possibly related to cell lysis) but the increase may not necessarily mean treatment failure. However, a consistent increase in tumour marker levels, coupled with lack of clinical improvement, may indicate treatment failure.
- Residual elevation after definitive treatment usually indicates persistent disease.
- Following tumour marker response is particularly useful when other evidence of disease is not readily accessible.
Monitoring for cancer recurrence
When monitoring these patients, tumour marker levels should be determined only when there is a potential for meaningful treatment.Tumour markers
| Tumour marker | Associated primary tumour | Other conditions which may yield positive results |
| CA 27.29 | Breast cancer. | Colonic, gastric, hepatic, lung, pancreatic, ovarian and prostate cancers. Breast, liver and kidney disorders, ovarian cysts. |
| CEA | Colorectal cancer. | Lung, gastric, pancreatic, breast, bladder cancers, medullary thyroid and other head and neck, cervical and hepatic cancers, lymphoma, melanoma. Cigarette smoking, peptic ulcers, inflammatory bowel disease, pancreatitis, hypothyroidism, cirrhosis, biliary obstruction. |
| CA 19-9 | Pancreatic and biliary tract cancers. | Colonic, oesophageal and hepatic cancers, pancreatitis, biliary disease, cirrhosis. |
| AFP | Hepatocellular carcinoma, nonseminomatous germ cell tumours. | Gastric, biliary and pancreatic cancers, cirrhosis, viral hepatitis, pregnancy. |
| Beta-hCG | Nonseminomatous germ cell tumours, gestational trophoblastic disease. | Rarely elevated in gastrointestinal cancers, hypogonadal states and marijuana use. |
| CA 125 | Ovarian cancer. | Endometrial, Fallopian tube, breast, lung, oesophageal, gastric, hepatic and pancreatic cancers, menstruation, pregnancy, fibroids, ovarian cysts, pelvic inflammation, cirrhosis, ascites, pleural and pericardial effusions, endometriosis. |
| PSA | Prostate cancer. | Prostatitis, benign prostatic hypertrophy, prostatic trauma, after ejaculation. |
- Measurement of both human chorionic gonadotrophin (hCG) and alpha-fetoprotein (AFP) is mandatory in patients in whom testicular or other germ cell cancers are strongly suspected (these markers are not raised in all such patients).
- Measurement of AFP and hCG is mandatory in the management of germ cell tumours.
- In some high-risk patients, measurement of AFP, CA 125 or CA 19-9 may aid early detection of hepatocellular carcinoma, ovarian cancer or pancreatic cancer.
- The positive predictive value of PSA levels in prostate cancer greater than 4 ng/mL is 20-30%. This rises to 50% when PSA levels exceed 10 ng/mL.
- Nevertheless, 20-30% of men with prostate cancer have PSA levels within normal ranges.
- Fewer than 2% of men with PSA levels below 20 ng/mL have bone metastases from prostate cancer.
CA 15-3 and CA 27.29 are markers used in breast cancer therapy monitoring. Both may be superseded by the estimation of circulating tumour cells (CTCs).
CA 15-3
- CA15-3 is useful in prognosis.
- CA 15-3 may also be raised in acute hepatitis, chronic liver diseases (eg, cirrhosis, chronic active hepatitis, chronic kidney disease, colitis and some skin conditions.
CA 27.29
- Has better sensitivity and specificity than CA 15-3.
- The CA 27.29 level is elevated in approximately 33% of women with early-stage breast cancer (stage I or II).
- It increases in women with late-stage disease (stage III or IV).
- CA 27.29 lacks predictive value in the earliest stages of breast cancer and so has no role in screening for or diagnosing the malignancy.
- It may be possible to detect asymptomatic recurrence (in patients at high risk - stage II or III) after curative treatment.
- CA 27.29 is specific and sensitive in detecting pre-clinical metastasis and this may lead to prompt imaging of probable sites of metastasis, possibly decreasing morbidity because of earlier treatment.
Cancer antigen 125 See separate Cancer Antigen 125 (CA 125) .
Alpha-fetoprotein See separate Alpha-fetoprotein (AFP) .
- AFP elevations are associated with hepatocellular carcinoma and nonseminomatous germ cell tumours.
- AFP levels are abnormal in 80% of patients with hepatocellular carcinoma and exceed 1,000 ng/mL in 40% of patients with this cancer. In conjunction with abdominal ultrasonography, it is recommended that AFP be measured at six-monthly intervals in patients at high risk of hepatocellular carcinoma (especially those with liver cirrhosis related to hepatitis B or hepatitis C).
- Other gastrointestinal cancers occasionally cause elevations of AFP but rarely to greater than 1,000 ng/mL. AFP may also be raised in patients with lung cancer.
- Patients with cirrhosis or viral hepatitis may have abnormal AFP values, although usually less than 500 ng/mL.
- Pregnancy also is associated with elevated AFP levels, particularly if the pregnancy is complicated by a spinal cord defect or other abnormality.
- Where AFP levels are elevated but no abnormality is found, there is a greater level of obstetric risk (also seen with hCG levels).
- Pregnancy.
- Germ cell tumours.
- Gestational trophoblastic disease.
- False positive levels occur in:
- Lung cancer
- Chronic kidney disease
- Menopause
- Hypogonadal states
- Marijuana use
Tumour markers are followed every one to two months for one year after treatment, then quarterly for one year and less frequently thereafter. AFP or beta-hCG elevation is frequently the first evidence of germ cell tumour recurrence.
Cancer antigen 19-9 Elevated levels of CA 19-9, an intracellular adhesion molecule, occur primarily in patients with pancreatic and biliary tract cancers but may also be raised in colorectal, gastric, hepatocellular, oesophageal and ovarian cancers.
- It has a sensitivity and specificity of 80-90% for pancreatic cancer.
- It has a sensitivity of 60-70% for biliary tract cancer.
- Benign conditions such as cirrhosis, cholestasis, cholangitis and pancreatitis also result in elevations, although values are usually less than 1,000 units per mL. May also be raised in diabetes mellitus and irritable bowel syndrome.
- CA 19-9 levels above 1,000 units per mL predict the presence of metastatic disease.
- Lack of sensitivity and specificity restricts the use of CA 19-9 measurement in the early diagnosis of pancreatic cancer but it may complement other diagnostic procedures, especially in the absence of cholestasis.
ThyroglobulinCan be used in detecting recurrence and monitoring treatment in patients with follicular or papillary thyroid cancer.
Paraproteins (M protein/Bence Jones' protein)
- Paraproteins can also be measured in urine.
- Can be used in the diagnosis, detecting recurrence and monitoring treatment in patients with B-cell proliferative disorders such as multiple myeloma.
Circulating methylated DNA Circulating nucleic acids may be biomarkers that could be used in the early detection of cancer. They could also be used to follow the progression of patients with cancer. Methylated DNA is one such nucleic acid-based marker. DNA is a very stable molecule and can be detected using simple polymerase chain reaction-based approaches.
No comments:
Post a Comment