All About Nutrition, essential Vitamins, essential Minerals and essential Amino-acids for a Maximum Health.
I love to discuss Nutrition Deficiencies and Benefits.
Deaths from COVID-19 dropped rapidly from a peak in late April to a low in May
A number of studies have suggested COVID-19 may taper off during the summer, due to higher humidity and other factors
A 1% decrease in humidity was predicted to increase the number of COVID-19 cases by 6.11%
COVID-19 disease severity is associated with vitamin D levels, with lower levels linked to more severe disease
If COVID-19 is seasonal, a resurgence is likely come fall, which is why the time for optimizing your vitamin D level is now
The U.S. Centers for Disease Control and Prevention’s provisional death counts for COVID-19 show a striking change. While starting at zero in February 2020 and spiking up to more than 5,000 deaths per week for the oldest age range (85 and over) and 111 among 25- to 34-year-olds in late April, they’ve plummeted.
There were 199 COVID-19 deaths for the week ending May 30, 2020, among those 85 and over, while only one death was reported among 25- to 34-year-olds — an extremely rapid decline from April to May.1 What happened to make the deaths come to a standstill, according to some experts, might be the same seasonal ebb and flow that happens with many respiratory infections: Summer may have killed it.
Many Respiratory Infections Decline in the Summer
While it’s possible to get respiratory infections like influenza any time of year, influenza is more common during the fall and winter, hence the “flu season” during those months. Respiratory syncytial virus (RSV), a leading cause of severe respiratory illness in young children and those aged 65 and over, is also more common in the fall and winter.
At least four common coronaviruses are also highly seasonal with transmission similar to influenza.2 Although these aren’t related to SARS-CoV-2, the virus that causes COVID-19, it is genetically related to the coronavirus responsible for the severe acute respiratory syndrome (SARS) outbreak of 2003.
This is notable because, as noted by professor Paul Hunter from the University of East Anglia in England, “Sars largely spread in hospitals but still died out in the summer in the Northern Hemisphere.”3 There are a number of reasons why SARS was quickly contained in about eight months, but the summer, with its higher temperature and humidity level, is among them.
What Makes Summer Less Conducive to Respiratory Infection?
Winter’s dry, cold air is favorable to the spread of flu transmission, and influenza spread is known to be affected by both temperature and humidity.4 During the winter, people also spend more time indoors, in enclosed spaces with less ventilation and less personal space compared to being outdoors in the summer.5
School is usually in session during the fall and winter, with students at home over the summer. School terms have been associated with higher transmission of respiratory viruses, while holidays lead to a 20% to 29% reduction in the rate at which influenza is transmitted in children.6 So, just the fact that children are in school in the winter may raise transmission rates.
What’s more, as noted by Marc Lipsitch, professor of epidemiology and director of the Center for Communicable Disease Dynamics at the Harvard T.H. Chan School of Public Health:7
“It is possible that the condition of the average person’s immune system is systematically worse in winter than summer. One hypothesis has focused on melatonin which has some immune effects and is modulated by the photoperiod, which varies seasonally. Another with more evidence is that vitamin D levels, which depend in part on ultraviolet light exposure (higher in summer) modulate our immune system in a positive way.”
Advertisement
Studies Suggest COVID-19 May Be Seasonal
A number of studies have suggested COVID-19 may, in fact, taper off during the summer. One preprint study tracked the seasonality of influenza viruses and endemic human coronaviruses over an eight-year period. The activity of human coronaviruses peaked the first week of January, with transmission facilitated by low indoor relative humidity (RH) of 20% to 30%.8
The researchers cited previous studies that found an increase in relative humidity to 50% reduced the transmission of both influenza and animal coronaviruses. What’s more, the study found a decrease in disease incidence by 50% in early March, 75% in early April and greater than 99% at the end of April. According to the study:9
“As a lipid-bound, enveloped virus with similar size characteristics to endemic human coronaviruses, SARS-CoV-2 should be subject to the same dynamics of reduced viability and transmission with increased humidity. In addition to the major role of social distancing, the transition from lower to higher indoor RH with increasing outdoor temperatures could have an additive effect on the decrease in SARS-CoV-2 cases in May.
Over the 8-year period of this study, human coronavirus activity was either zero or >99% reduction in the months of June through September, and the implication would be that SARS-Cov-2 may follow a similar pattern.”
Humidity May Be a Major Factor
A study conducted in Sydney, Australia, found a similar connection between humidity and COVID-19. A 1% decrease in humidity was predicted to increase the number of cases by 6.11%,10 with researchers stating, “During periods of low relative humidity, the public health system should anticipate an increased number of COVID‐19 cases.”11
Professor Michael Ward, an epidemiologist in the Sydney School of Veterinary Science at the University of Sydney, said in a news release that humidity appeared to be a major factor:12
"When it comes to climate, we found that lower humidity is the main driver here, rather than colder temperatures. It means we may see an increased risk in winter here, when we have a drop in humidity. But in the northern hemisphere, in areas with lower humidity or during periods when humidity drops, there might be a risk even during the summer months.
… When the humidity is lower, the air is drier and it makes the aerosols smaller. When you sneeze and cough those smaller infectious aerosols can stay suspended in the air for longer. That increases the exposure for other people. When the air is humid and the aerosols are larger and heavier, they fall and hit surfaces quicker."
Aside from affecting transmission rates, humidity may also affect the survival of viruses. The addition of a portable humidifier with an output of 0.16 kilograms of water per hour in the bedroom increased absolute humidity 11% and relative humidity 19% during sleeping hours compared to having no humidifier present, according to one study. Along with the increases in humidity came a decrease in the survival of influenza virus, by 17.5% to 31.6%.13
Humidity even influences innate immune defenses against viral infections. In an animal study, dry air compromised the mice’s resistance to infection, and those housed at lower humidity levels had impaired mucociliary clearance, innate antiviral defense and tissue repair function, the study found.14
The Vitamin D Connection
The other reason why summer may slash COVID-19 deaths is because summer equals greater exposure to sunlight, which boosts vitamin D levels. There is strong scientific evidence vitamin D plays a central role in your immune response and your ability to fight infections. It’s been shown in an analysis of 212 people with lab-confirmed COVID-19 that disease severity is associated with vitamin D levels, with lower levels linked to more severe disease.15
A review published in the journal Nutrients also concluded that not only could vitamin D be useful to reduce the risk of infection with COVID-19, but also could be helpful for treatment:16
“Evidence supporting the role of vitamin D in reducing risk of COVID-19 includes that the outbreak occurred in winter, a time when 25-hydroxyvitamin D (25(OH)D) [vitamin D] concentrations are lowest; that the number of cases in the Southern Hemisphere near the end of summer are low; that vitamin D deficiency has been found to contribute to acute respiratory distress syndrome; and that case-fatality rates increase with age and with chronic disease comorbidity, both of which are associated with lower 25(OH)D concentration.”
If COVID-19 is seasonal, a resurgence is likely come fall, which is why the time for optimizing your vitamin D level is now. To improve your immune function and lower your risk of viral infections, you’ll want to raise your vitamin D to a level between 60 nanograms per milliliter (ng/mL) and 80 ng/mL by fall. In Europe, the measurements you’re looking for are 150 nanomoles per liter (nmol/L) and 200 nmol/L.
Why Do so Many Experts Get It Wrong?
Harvard professor Lipsitch is among those who said COVID-19 would “probably not” go away on its own in warmer weather. “The short answer is that while we may expect modest declines in the contagiousness of SARS-CoV-2 in warmer, wetter weather and perhaps with the closing of schools in temperate regions of the Northern Hemisphere, it is not reasonable to expect these declines alone to slow transmission enough to make a big dent,” he said.17
CDC’s provisional death counts appear to suggest otherwise, but some have cautioned that COVID-19 is too new to be seasonal. In other words, because fewer people have established immunity, a new virus has an advantage in that it can thrive even in less-than-optimal conditions for a virus, i.e., the summer.
“Old viruses,” Lipsitch said, “which have been in the population for longer, operate on a thinner margin — most individuals are immune, and they have to make do with transmitting among the few who aren’t.”18
Likewise, a study in Science used a computer model to suggest that while COVID-19 may fall into seasonal patterns eventually, this may not occur until more people develop immunity, noting that “susceptible supply” is limiting the role of climate in the early COVID-19 pandemic.19
The drastic decline in COVID-19 deaths that occurred from April to May do suggest a seasonal component, but what’s driving the drop is not completely understood. It’s likely a combination of humidity, heat, human behaviors, vitamin D levels and, likely, other aspects of sunlight exposure that are culminating in this decline.
With summer upon us in the U.S., you can use it to your advantage to spend time outdoors, optimize your vitamin D levels and get sensible sun exposure, all of which can help you support health and reduce your susceptibility to viral infections.
DHA, a type of
omega-3, is a major structural component of the retina of your eye.
When you don't
get enough DHA, vision problems may arise.
Interestingly,
getting enough omega-3 is linked to a reduced risk of macular degeneration, one
of the world's leading causes of permanent eye damage and blindness.
Summary
An omega-3 fatty acid called DHA is a major
structural component of your eyes’ retinas. It may help prevent macular
degeneration, which can cause vision impairment and blindness.
Omega-3s are
crucial for brain growth and development in infants.
DHA accounts for
40% of the polyunsaturated fatty acids in your brain and 60% in the retina of
your eye.
Therefore, it's
no surprise that infants fed a DHA-fortified formula have better eyesight than
infants fed a formula without it.
Getting enough
omega-3s during pregnancy is associated with numerous benefits
for your child, including:
Higher
intelligence
Better
communication and social skills
Fewer
behavioral problems
Decreased
risk of developmental delay
Decreased
risk of ADHD, autism and cerebral palsy
Summary
Getting enough omega-3s during pregnancy and early
life is crucial for your child’s development. Supplementing is linked to higher
intelligence and a lower risk of several diseases.
Heart attacks
and strokes are the world's leading causes of death.
Decades ago,
researchers observed that fish-eating communities had very low rates of these
diseases. This was later linked to omega-3 consumption.
Since then,
omega-3 fatty acids have been tied to numerous benefits for heart health
These benefits
address:
Triglycerides:
Omega-3s can cause a major reduction in triglycerides, usually in the range of 15–30% .
Blood
pressure: Omega-3s can reduce blood pressure levels in people
with high blood pressure.
“Good”
HDL cholesterol: Omega-3s can raise “good” HDL
cholesterol levels.
Blood
clots: Omega-3s can keep blood platelets from clumping
together. This helps prevent the formation of harmful blood clots.
Plaque:
By keeping your arteries smooth and free from damage, omega-3s help prevent the
plaque that can restrict and harden your arteries.
Inflammation:
Omega-3s reduce the production of some substances released during your body’s
inflammatory response.
For some people,
omega-3s can also lower “bad” LDL cholesterol. However, evidence is mixed —
some studies find increases in LDL.
Despite these
beneficial effects on heart disease risk factors, there is no convincing
evidence that omega-3 supplements can prevent heart attacks or strokes. Many
studies find no benefit.
Summary
Omega-3s improve numerous heart disease risk
factors. However, omega-3 supplements do not seem to reduce your risk of heart
attacks or strokes.
Attention
deficit hyperactivity disorder (ADHD) is a behavioral disorder characterized by
inattention, hyperactivity and impulsivity.
Several studies
note that children with ADHD have lower blood levels of omega-3 fatty acids
than their healthy peers.
What's more,
numerous studies observe that omega-3 supplements can reduce the symptoms of
ADHD.
Omega-3s help
improve inattention and task completion. They also decrease hyperactivity,
impulsiveness, restlessness and aggression.
Recently,
researchers observed that fish oil supplements were one of the most promising
treatments for ADHD .
Summary
Omega-3 supplements can reduce the symptoms of ADHD
in children. They improve attention and reduce hyperactivity, impulsiveness and
aggression.
It includes
central obesity — also known as belly fat — as well as high blood pressure, insulin resistance, high triglycerides and low
“good” HDL cholesterol levels.
It is a major
public health concern because it increases your risk of many other illnesses,
including heart disease and diabetes.
Omega-3 fatty
acids can improve insulin resistance, inflammation and heart disease risk
factors in people with metabolic syndrome .
Summary
Omega-3s can have numerous benefits for people with
metabolic syndrome. They can reduce insulin resistance, fight inflammation and
improve several heart disease risk factors.
Inflammation is
a natural response to infections and damage in your body. Therefore, it is
vital for your health.
However,
inflammation sometimes persists for a long time, even without an infection or
injury. This is called chronic — or long-term — inflammation.
Long-term
inflammation can contribute to almost every chronic Western illness, including
heart disease and cancer .
Notably, omega-3
fatty acids can reduce the production of molecules and substances linked to
inflammation, such as inflammatory eicosanoids and cytokines .
Studies have
consistently observed a connection between higher omega-3 intake and reduced inflammation .
Summary
Omega-3s can reduce chronic inflammation, which can contribute to heart
disease, cancer and various other diseases.
In autoimmune
diseases, your immune system mistakes healthy cells for foreign cells and
starts attacking them.
Type 1 diabetes
is one prime example, in which your immune system attacks the insulin-producing
cells in your pancreas.
Omega-3s can
combat some of these diseases and may be especially important during early
life.
Studies show
that getting enough omega-3s during your first year of life is linked to a
reduced risk of many autoimmune diseases, including type 1 diabetes, autoimmune
diabetes and multiple sclerosis .
Omega-3s also
help treat lupus, rheumatoid arthritis, ulcerative colitis, Crohn's disease and
psoriasis .
Summary
Omega-3 fatty acids can help fight several
autoimmune diseases, including type 1 diabetes, rheumatoid arthritis,
ulcerative colitis, Crohn's disease and psoriasis.
Cancer is one of the leading causes of death in
the Western world, and omega-3 fatty acids have long been claimed to reduce the
risk of certain cancers.
Interestingly,
studies show that people who consume the most omega-3s have up to a 55% lower
risk of colon cancer .
Additionally,
omega-3 consumption is linked to a reduced risk of prostate cancer in men and
breast cancer in women. However, not all studies give the same results .
Summary
Omega-3 intake may decrease the risk of some types
of cancer, including colon, prostate and breast cancer.
Osteoporosis and
arthritis are two common disorders that affect
your skeletal system.
Studies indicate
that omega-3s can improve bone strength by boosting the amount of calcium
in your bones, which should lead to a reduced risk of osteoporosis
Omega-3s may
also treat arthritis. Patients taking omega-3 supplements have reported reduced
joint pain and increased grip strength .
Summary
Omega-3s may improve bone strength and joint health, potentially reducing your
risk of osteoporosis and arthritis.
Menstrual pain
occurs in your lower abdomen and pelvis and often radiates to your lower back
14.
Omega-3s May Improve Bone and Joint Health
Osteoporosis and
arthritis are two common disorders that affect
your skeletal system.
Studies indicate
that omega-3s can improve bone strength by boosting the amount of calcium
in your bones, which should lead to a reduced risk of osteoporosis .
Omega-3s may
also treat arthritis. Patients taking omega-3 supplements have reported reduced
joint pain and increased grip strength .
Summary
Omega-3s may improve bone strength and joint health, potentially reducing your
risk of osteoporosis and arthritis.
15.
Omega-3s Can Alleviate Menstrual Pain
Menstrual pain
occurs in your lower abdomen and pelvis and often radiates to your lower back
and thighs.
It can
significantly affect your quality of life.
However, studies
repeatedly prove that women who consume the most omega-3s have milder menstrual
pain .
One study even
determined that an omega-3 supplement was more effective than ibuprofen in
treating severe pain during menstruation .
Summary
Omega-3 fatty acids can reduce menstrual pain and
may even be more effective than ibuprofen, an anti-inflammatory drug.
Managing
oil production and hydration of your skin.
Preventing
hyperkeratinization of hair follicles, which appears as the little red bumps
often seen on upper arms.
Reducing
premature aging of your skin.
Reducing
the risk of acne.
Omega-3s can
also protect your skin from sun damage. EPA helps block the release of
substances that eat away at the collagen
in your skin after sun exposure.
Summary
Omega-3s can help keep your skin healthy,
preventing premature aging and safeguarding against sun damage.
In summary, depressed mood may simply be a sign of magnesium deficiency in the brain. Boosting brain magnesium levels, particularly with the use of magnesium L-threonate, may have profound benefits on mood.
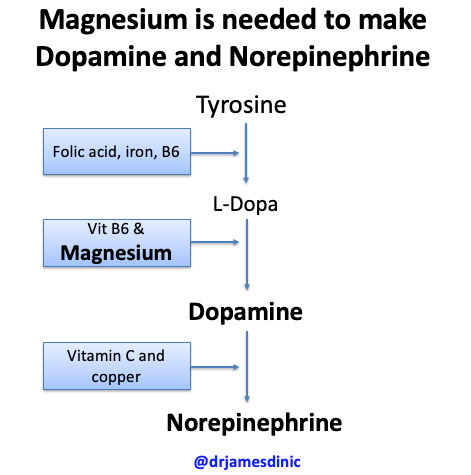
Importantly, magnesium is needed to make the three primary neurotransmitters in the brain, i.e., serotonin, dopamine and noradrenaline and melatonin which is important for sleep.
2019 (COVID-19), with a clinical outcome ranging from mild to severe, including death. To date,
it is unclear why some patients develop severe symptoms. Many authors have suggested the
involvement of vitamin D in reducing the risk of infections; thus, we retrospectively investigated the
25-hydroxyvitamin D (25(OH)D) concentrations in plasma obtained from a cohort of patients from
Switzerland. In this cohort, significantly lower 25(OH)D levels (p = 0.004) were found in PCR-positive
for SARS-CoV-2 (median value 11.1 ng/mL) patients compared with negative patients (24.6 ng/mL); his was also confirmed by stratifying patients according to age >70 years. On the basis of this preliminary observation, vitamin D supplementation might be a useful measure to reduce the risk of
infection. Randomized controlled trials and large population studies should be conducted to evaluate
these recommendations and to confirm our preliminary observation.
(COVID-19), with clinical outcomes ranging from mild to severe, including death. To date, there is
no specific recommended treatment, with COVID-19- and SARS-COV-2-a ected patients targeted to
receive supportive care to help relieve symptoms.
However, only a fraction of infected people show clinical symptoms, and an even lower percentage
require medical attention [1,2]. To date, it is not yet known why some patients develop more
severe symptoms.
Recently, some articles have suggested the possible involvement of vitamin D in reducing the risk
of respiratory tract infections, especially in the influenza and COVID-19 context. Furthermore, the
role of vitamin D supplementation in reducing the risk of infection [3–6] is still under investigation,
however, no clinical evidence has been reported yet.
For these reasons, we retrospectively described the 25-hydroxyvitamin D (25(OH)D) plasma
concentrations in a cohort of patients from Switzerland.